

Most claims about PDRN sound bold, but not all delivery methods match the hype. Some clinics promote injections as the only serious option. Some brands push creams as a full replacement. The truth sits between those two claims.
Topical PDRN and injectable PDRN do not compete in a simple way. They reach different depths, act at different speeds, and fit different patients. Any clinic that understands this can plan treatments with far better results.
This guide looks at how each route works in real skin. It also explains when one method is clearly better, and when a smart mix gives the best value.
What PDRN Is Actually Doing In The Skin
PDRN stands for polydeoxyribonucleotide, a chain of DNA fragments. Most medical PDRN comes from salmon DNA that is purified to a high standard.
In skin, PDRN supports repair in two main ways.
- It activates the A2A adenosine receptor, which calms local inflammation and supports healing.
- It provides DNA building blocks that fast growing cells can reuse.
Readers who want a deeper science review can study the article on what PDRN is and how it works. Understanding these fundamental mechanisms helps explain why delivery depth matters so much for clinical outcomes.
Those effects do not change with the delivery route. What changes is how much PDRN reaches the target layer, and how long it stays active there. This distinction is critical for both patient selection and treatment planning.
How Far Topical PDRN Can Really Go
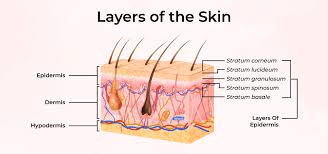
Topical PDRN sits in creams, serums, or masks. The main limit is the skin barrier. Intact stratum corneum keeps most large molecules out, and PDRN fragments are relatively large compared to typical cosmetic actives.
Clinical data on exact penetration is still limited. Current work suggests that topical PDRN mainly stays in the epidermis. Some very small fragments may reach the upper dermis, but the share is likely low.
That means topical PDRN is better for surface focused goals. Examples include support of barrier repair after peels and improved texture with mild fine lines. A detailed review of this issue appears in the article on maximizing topical PDRN absorption.
Topical use has three clear strengths:
- Low risk, with rare reports of strong reactions.
- Easy home use, which helps with long term care.
- Good fit after clinic work, to support healing.
The trade off is clear. Topical PDRN will not give the same depth of change as a course of injections. For patients seeking meaningful improvements in mature skin collagen and elasticity, injectable delivery typically proves necessary.
What Injection PDRN Does That Creams Cannot
Injection PDRN bypasses the barrier and places the product in the dermis. That is where fibroblasts sit, and where most collagen change takes place.
Most studies that support clear gains in elasticity, fine lines, and acne scars use injection protocols. They often report more clear changes in texture compared with topicals, particularly when PDRN accelerates wound healing in deeper tissue layers.
An overview of these trials and their quality is covered in the article on PDRN clinical efficacy and data. The consistent finding is that direct dermal delivery produces more substantial and measurable tissue changes.
Clinics that use PDRN injections see three main advantages.
- Higher local dose at the correct depth.
- More clear collagen support in photoaged skin.
- Better impact on scars and deeper wrinkles.
The clear cost is discomfort and down time. Some protocols use many micro injections. Mild swelling and bruising are common for a few days. For patients considering this route, understanding PDRN aftercare essentials helps set realistic recovery expectations.
What Current Comparisons Actually Show
Two detailed clinic pieces from Singapore review topical PDRN versus injection based care. Both note that current topical formulas do not fully replace injection based protocols for deep rejuvenation.
The authors state that topical PDRN may support skin quality, but that injections still lead for structural change in the dermis.
These views appear in public clinic reviews on topical versus injectable PDRN skincare and a related review of topical PDRN versus Korean PN injections.
The key idea is simple. Topical care is support. Injection care is core treatment when a patient seeks clear lifting of lines and texture. This distinction aligns with broader observations about PDRN’s role in reversing sun damage, where dermal repair drives visible improvement.
When Topical PDRN Is The Better Tool
Topical PDRN is not a weak option. It is just a different tool. It fits best in cases like these.
1. Maintenance after a full injection series
After a full course of injections, collagen change continues for months. Topical PDRN can help protect the barrier and calm mild inflammation during that period.
It also suits patients who do not want more needles soon, but still want to protect gains. For those managing sensitive skin with anti-inflammatory needs, topical application offers ongoing support without repeated invasive procedures.
2. Support for sensitive or very dry skin
Barrier impaired skin reacts poorly to strong actives. Topical PDRN can support repair with less risk of stinging than high strength acids or retinoids.
Patients with chronic dryness or mild eczema often accept this type of care more easily. The gentle nature of topical PDRN makes it particularly valuable when PDRN calms inflammatory skin responses without triggering additional irritation.
3. Bridge care with other energy devices
Many clinics pair PDRN with lasers or radiofrequency. Injection at each visit is not always needed. Topical PDRN can serve as a bridge between strong sessions.

Readers who plan complex mix protocols can study PDRN in aesthetic medicine practice for ideas. The integration of topical support between injectable sessions often optimizes overall treatment outcomes.
When Injection Clearly Wins
For deeper problems, topical PDRN will not match injection care. Some clear examples follow, where understanding patient selection for PDRN becomes critical.
- Photoaging with clear dermal thinning. Sun damage with etched lines needs support in the dermis. PDRN injections can work with other tools to restore structure.
- Atrophic acne scars. Topical care may smooth texture a little, but most real gains need needles. PDRN injections, often with microneedling or subcision, can support better repair.
- Marked laxity on hands. Thin hand skin needs deeper support. A focused guide on this topic is given in the article on PDRN for hand rejuvenation.
In each case, the common point is clear. The main target is not the barrier. The target is the dermis and sometimes deeper. This requirement explains why PDRN for stretch marks and body rejuvenation typically requires injectable protocols for meaningful results.
Safety, Regulation, And Product Quality
Topical and injectable PDRN also differ in how they are regulated. Understanding these distinctions helps practitioners navigate legal compliance and patient safety.
Topical PDRN creams often sit in the cosmetic space. This means there is less formal review of clinical effect, and more focus on safety for surface use.
Injectable PDRN products often sit closer to medical device or drug rules, depending on the region. This usually means tighter control of purity and clear use protocols.
Readers who need a wider view of these issues can refer to the guide on PDRN global regulatory status. For clinics, quality control has two clear parts.
- Product sourcing from trusted, audited makers.
- Protocol design that fits current evidence, not trends.
Topical products can vary a lot in PDRN grade and actual content. That is why clinics should ask for clear data before adding new lines. Understanding PDRN shelf life, storage, and handling ensures product integrity regardless of delivery format.
How Skilled Clinics Combine Topical And Injection
The most effective use of PDRN does not treat topical and injection care as rivals. Strong clinics use both as parts of a clear plan.
A common pattern looks like this:
- A series of injection sessions for core change in texture.
- Targeted work with microneedling or lasers for scars or spots.
- Daily topical PDRN for barrier support and comfort between visits.
This type of multi step approach is described in more detail in the guide on PDRN with microneedling and combination results. The integration of both delivery methods often proves superior to either approach alone.
In that context, topical PDRN stops being a weak copy of injection care. It becomes an important part of the healing phase. Some clinics even incorporate PDRN and Botox combination treatments where topical support enhances recovery between injectable sessions.
For practitioners seeking to refine technique across both formats, PDRN training and certification often covers optimal integration strategies for topical and injectable protocols.
So Which Delivery Method Wins?
If the goal is clear lifting of wrinkles and scars, injection PDRN is still the leading choice. It places active material where it can act on collagen and deeper repair, particularly when combining PDRN with fillers safely for comprehensive facial rejuvenation.
If the goal is gentle support, barrier repair, and comfort during longer plans, topical PDRN is a valuable tool. It is safer for home use and easier to keep up. The market trends and regulatory outlook suggest growing sophistication in both topical and injectable product development.
Clinics that treat these routes as partners, not rivals, will give better care. The real winner is not a single method. The winner is a clear protocol that uses the right form of PDRN at the right depth, for the right goal.
Understanding microdosing PDRN techniques offers additional refinement possibilities for practitioners seeking to optimize delivery precision across both topical and injectable approaches.